
Clinical-Stage · Maternal-Fetal Medicine
Redefining Outcomes
in Early-Onset Preeclampsia
A first-in-class, fetal-sparing complement therapeutic built to change the trajectory of early-onset preeclampsia.
Clinical-Stage · Maternal-Fetal Medicine
A first-in-class, fetal-sparing complement therapeutic built to change the trajectory of early-onset preeclampsia.
Nesya targets the “Why” of early-onset preeclampsia, upstream complement activation, rather than the “What” of downstream sFlt-1/PlGF imbalance. One disciplined program, built to answer a decisive clinical question.
The Problem
Early-onset preeclampsia (EOPEC) is a severe, fast-progressing maternal-fetal disease. Today the sole definitive intervention is delivering the placenta, which, before term, means a premature baby.
Maternal organ injury, hypertension, and seizure risk can escalate within hours, an inpatient, high-acuity emergency.
Management is monitoring, blood-pressure control, and timing delivery. Nothing modifies the underlying disease.
Ending the pregnancy “treats” the mother but delivers a premature infant into the NICU, trading one harm for another.
Source: DelveInsight, diagnosed preeclampsia prevalence across the 7MM, 2024.
The Science
Complement, an immune pathway triggered by placental debris, initiates and amplifies early-onset preeclampsia. Rare inherited C5 and C6 variants that track with the disease support it as a likely driver, not just a correlation.
Driven by fetoplacental debris
Inflammation & ischemia
Angiogenic imbalance
EOPEC manifestations
The Solution
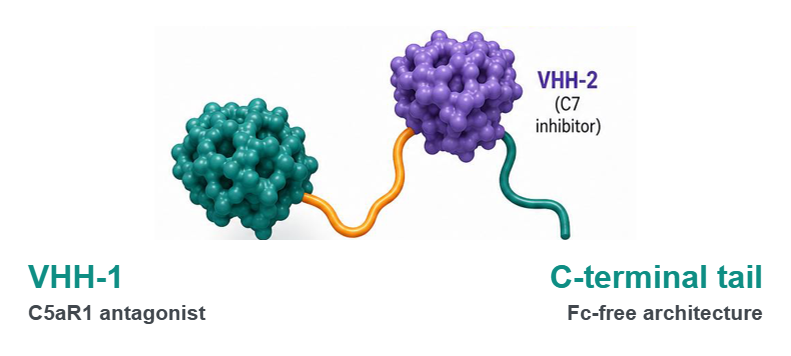
Designed to remain on the maternal side of the interface. Standard antibodies carry a kind of “passport”, the Fc region, that lets them cross the placenta. Elaranen is built Fc-free, intended to minimize placental transfer and keep activity on the mother’s side.
No Fc domain means no FcRn-mediated transport across the placenta, the property that lets antibodies reach the fetus.
VHH-1 mitigates maternal systemic inflammation and clinical symptoms; VHH-2 mitigates placental injury and decreases the release of fetal placental debris.
Eculizumab is known to cross the placenta. Elaranen’s bispecific VHH (C5aR1 + C7) architecture is designed to avoid that.
Why Now
The science, the capital, and the technology have arrived, and the upstream complement lane has no dedicated clinical entrant.
Bench and translational studies demonstrate complement activation precedes angiogenic imbalance and contributes to placental injury.
Top-tier venture syndicates are now backing disease-modifying preeclampsia programs, establishing PEC as an investable therapeutic category.
Modern nanobody engineering enables maternally-restricted, fetal-sparing designs.
Every competitor is downstream; the upstream lane has no dedicated clinical entrant.
The Team

A practicing maternal-fetal medicine specialist with decades of direct EOPEC clinical experience, who designed Nesya’s complement strategy from clinical first principles.

Operational expertise, responsible for execution and company building, turning a defined asset into a financeable, IND-directed program.
Why Us
No team is better positioned to run the decisive complement test in EOPEC: clinical origin, a real human signal, and a defined, translation-ready asset.
Career Maternal-Fetal Medicine specialist who founded a dedicated complement research unit at Harvard.
His own 2013 cases were the first to show complement blockade prolonging pregnancy in HELLP.
He filed a complement patent for preeclampsia in 2005, 20 years early.
Not a concept: a FASTA-locked, owned bispecific VHH ready to advance.
A defined path to human placental-perfusion rescue, the strongest pre-trial signal.

Nesya is executing the decisive clinical test. For investment, partnership, or media inquiries, get in touch.
We've received your inquiry and will reply within two business days at the email you provided.